|
Autor:
Ernest E. Moore, M.D.
Denver, Colorado, USA |
|
|
|
BLOOD SUBSTITUTES IN TRAUMA CARE |
The current generation of
blood substitutes employed in clinical
trials are fundamentally red blood cell
(RBC) substitutes; i.e., they are designed
primarily to transport oxygen. The products
that are now being tested in advanced phase
clinical trials are derived from hemoglobin
and often referred to as hemoglobin based
oxygen carriers (HBOCs). The potential
clinical benefits of HBOCs are well known.
The objectives of this brief overview are to
outline potential clinical applications in
trauma care and review the results of HBOCs
in recent patient trials.
Potential Role of
Hemoglobin-Based Oxygen Carriers in Trauma
Care
FDA approval of a new product
proceeds through phase I, II, and III
studies designed to establish safety and
efficacy. FDA regulation defines efficacy
as? a reasonable expectation that. .
.pharmacologic or other effects of the
biologic product. . .will serve a chemically
significant function in the diagnosis, cure,
mitigation, treatment or prevention of
disease in man.? The Center for Biologics
Evaluation and Research (CBER) is the review
body for the FDA in the arena of biologies
and has published a comprehensive listing of
?points to consider in the safety and
efficacy assessment of HBOCs.? Specific
recommendations for clinical studies were in
three areas: perioperative applications,
acute hemorrhagic shock, and regional
perfusion. Field trials for severe trauma,
where RBCs are not available, were warned as
difficult because of safety and ethical
issues. Decreased perioperative allogeneic
RBC transfusion was regarded as a clinical
benefit, but the potential risks of HBOCs
would have to be defined and evaluated as
well.
Clinical Evaluation of
Modified Tetrameric Hemoglobin in Trauma
Care
Of the modified Hb tetrameric
solutions that looked promising in the late
1980s, only one formulation was authorized
by the FDA for a phase III study in trauma.
HemAssist (Baxter Healthcare, Boulder, CO)
consisted of Hb tetramers crossed linked
between alpha subunits with bis 3,5
diabromosalicyl fumarate to prevent
dissociation into dimers and reduce oxygen
affinity. Unfortunately this product failed.
Regarded by some as a major setback for the
clinical implementation of HBOCs, it is
important to emphasize that this US
multicenter trial of diaspirin cross-linked
Hb (DCLHb) for the treatment of severe
traumatic hemorrhagic shock was based on the
explicit proposal that ?DCLHb was tested not
as a substitute for blood but rather as an
adjunct to the currently used therapies for
enhancing oxygen delivery: fluids, blood,
and operative intervention.? Although an
unexpected outcome raises the issue of
comparable study groups, the difference in
the primary study endpoint was concerning:
the 28-day mortality for the DCLHb group was
46% (24 of 52), compared with 17% for the
control (normal saline) group (8 of 46).
Clinical Safety of
Polymerized Hemoglobin in Trauma Care
At this moment, the most
promising HBOCs clinically are polymerized
Hb solutions. Perhaps a coincidence but
polymerization addresses several of the
problems inherent in tetrameric Hb; i.e.,
enhanced intravascular retention and reduced
colloid osmotic activity. Polymerization
also appears to attenuate vasoconstriction
associated with the infusion of Hb
solutions. A proposed explanation is that
tetrameric Hb (65 KDa) extravasates through
the endothelium to bind abluminal NO,
leading to unopposed vasoconstriction; but
polymerized Hb (>130 KDa) remains in the
vasculature to bind only luminal NO.
Polymerized HBOCs have undergone extensive
preclinical and clinical testing for safety.
Hemopure (Biopure Corp,
Cambridge, MA), a polymer of bovine Hb, has
been used successfully to reduce allogeneic
RBC transfusion in elective cardiac, aortic,
and hepatic surgery. Animal
studies designed to replicate prehospital
hypotensive resuscitation for hemorrhagic
shock have also been encouraging although
the issue of compromised tissue perfusion
because of vasoconstriction has surfaced.
Hemopure has been approved for replacement
of acute blood loss in South Africa, but
there are no published results to date.
PolyHeme (Northfield lab, Evanston, IL) has
been the only product to be evaluated in
trauma patients to date. Under FDA guidance,
we initiated clinical trials in trauma to
confirm safety with escalating doses of
PolyHeme. Cognizant of the vasoconstriction
associated with the DCLHb clinical trial, we
designed a study to specifically evaluate
the pulmonary vascular response to PolyHeme
infusion in acutely injured patients.
Clinical Efficacy of
Polymerized Hemoglobin in Trauma Care
Perioperative Applications:
Reduce Allogeneic RBC Transfusions in Trauma
Care
Prompted by FDA guidelines to
demonstrate efficacy, all HBOC companies
have pursued what appears to be the simplest
clinically; i.e., to reduce the need for
allogeneic RBC transfusions. In
collaboration with David B Hoyt, MD, we
conducted a randomized trial in patients
requiring urgent transfusion. The total
number of allogeneic RBC transfusions for
the control versus PolyHeme was 10.4
+ 0.9 units versus 6.8 + 0.9
units (p < 0.05), respectively, through day
1, and 11.3 + 0.9 units versus
7.8
+ 0.9 units (p = 0.06), respectively,
through day 3. With our long-term interest
in the pathogenesis of postinjury MOF, we
then pursued the hypothesis that PolyHeme,
in lieu of stored RBCs during initial
resuscitation, would attenuate the adverse
immunoinflammatory effects of allogeneic RBC
transfusion. In preparation for these
clinical trials, we conducted in vitro
studies to test our hypothesis. The plasma
fraction from three or more units of stored
RBCs primed the human PMNs for enhanced
superoxide production and elastase release
but this was not seen with equivalent
volumes of PolyHeme. In our subsequent
clinical trial, circulating PMNs from
patients resuscitated with stored RBCs
manifested evidence of priming through
increased CD11b/CD18 expression and enhanced
superoxide production. Furthermore, patients
resuscitated with stored RBCs had higher
levels of the proinflammatory cytokines IL6
and IL8, and higher levels of the
counterregulatory cytokine IL10.
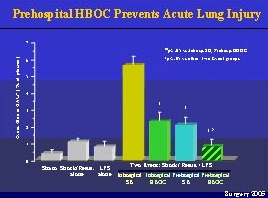
Acute Hemorrhagic Shock: When
Stored RBCs are Unavailable in Trauma Care
The most compelling
indication for an HBOC is the scenario in
which stored RBCs are unavailable. This
potential benefit for military use has
largely driven the development of HBOCs, but
there are also a number of key applications
in civilian trauma care. Despite the appeal,
the scientific design and ethical conduct of
clinical trials to establish efficacy of
HBOCs when RBCs are unavailable remain a
challenge. To best approximate this
scenario, we compared the 30-day mortality
in 171 trauma patients given up to 20 units
(1,000 g) of PolyHeme, compared with a
historic control of 300 surgical patients
who refused stored RBCs on religious
grounds. The 30-day mortality was 25.0% (10
of 40 patients), compared with 64.5% (20 of
31 patients) in the control patients.
With this background, a large
multicenter prehospital trial was initiated
in the U. S. in January 2003. Severely
injured patients, blunt or penetrating, with
a SBP
< 90 mm Hg due to acute blood
loss are randomized at the scene to receive
either the standard crystalloid
resuscitation or PolyHeme. The study is
conducted, by necessity, with exception to
informed consent. In the hospital, the
control group receives stored RBCs as needed
while the study group is administered
PolyHeme up to six units and then stored
RBCs as needed. The primary study endpoint
is 30 day mortality; the secondary endpoints
include incidence of ARDS and MOF as well as
amount of stored RBC transfusion. At this
moment, 25 trauma centers in the US are
participating in this trial projected for
720 patients. The final interim analysis of
500 patients enrolled to date is in progress
today.
|