|
Autor:
Ernest E. Moore, M.D.
Denver, Colorado, USA |
|
|
|
RETROPERITONEAL PACKING AS A
RESUSCITATION TECHNIQUE FOR
HEMODYNAMICALLY UNSTABLE PELVIC
FRACTURE
|
The optimal management strategy for
unrelenting hemorrhage produced by unstable
pelvic fractures remains controversial. The
basic cornerstones of modern pelvic fracture
management in North America are early
identification, resuscitation with blood and
blood products, treatment of associated
injuries and control of pelvic bleeding with
a combination of mechanical stabilization
and arterial embolization. The published
European approach has emphasized packing of
the pelvis through an abdominal approach and
direct arterial control instead of
angiography.
Considering that >85% of bleeding from major
pelvis fractures is venous in origin, we
have recently used mechanical stabilization
followed by direct retroperitoneal packing
to control life-threatening hemorrhage due
to unstable pelvic fractures arriving to the
hospital in hemorrhagic shock. To our
knowledge, direct packing via a
retroperitoneal approach to control pelvic
fracture bleeding has not been previously
reported in North America. We present two
illustrative cases. Although the injury
mechanisms and fracture patterns were
disparate, both patients survived emergent
operative intervention relying on
retroperitoneal packing with C-clamp
reduction of the pelvic volume. Herein, we
discuss the acute management of these
patients, and provide a detailed technical
description of the key operative maneuvers.
Case 1
S.W. is a 48 year-old male line worker who
sustained an unrestrained fall of
approximately fifty feet from a power line.
He was initially transported and treated at
an outlying facility for hemodynamic
instability from a mechanically unstable
pelvic fracture with a presenting blood
pressure (BP) of 84/40 mmHg. He remained
hemodynamically unstable with a systolic
blood pressure (SBP) less than 90 mmHg
despite having his pelvis bound with a sheet
and receiving two units of packed red blood
cells (PRBCs).
On arrival to our center, the patient’s BP
was 104/70 mmHg with a pulse of 154/min.
Laboratory values included a base deficit of
-11 meq/L. Ultrasound examination was
negative for free fluid in the abdomen.
Trauma anteroposterior radiographs of the
pelvis showed a Young and Burgess APC III
fracture and a right Denis type II sacral
fracture. Despite receiving an additional
two units of PRBCs, the patient continued to
have tachycardia greater than 150/min and
the blood pressure decreased to 80/40. He
was taken emergently to the operating room
for external fixation with a C-clamp and
pelvic packing. A C-clamp (DePuy, Warsaw,
IN) was placed in the posterior position as
described by Browner without fluoroscopic
imaging. The retroperitoneum was then opened
via an 8cm midline incision. Venous bleeding
was noted coming from the right posterior
pelvis. the true pelvis was directly packed
using our proposed technique. The total time
for the operative procedure was 22 minutes.
The patient departed the operating room 67
minutes after his arrival in the emergency
department.
The patient was taken to the surgical
intensive care unit for further
resuscitation. At ninety-six hours
post-admission the patient underwent
definitive pelvic surgery with anterior and
posterior fixation. He received a total of
six units of PRBCs and was discharged from
the hospital after 13 days to a
rehabilitation facility with normal
cognitive functioning.
Case 2
J.R. is a ten year-old male who was thrown
from a horse and dragged for approximately
fifty feet before being extricated. He was
emergently transported to an outside
facility via air evacuation; and intubated
enroute; he had a right femoral shaft
fracture and an open pelvis fracture. His
lab values included a base deficit of -10
meq/L. Treatment at the outside hospital
consisted of administration of two units of
PRBCs, two units of FFP and binding of his
pelvis with a sheet.
On arrival at our center the patient’s vital
signs were a SBP of 90 mmHg and a pulse of
128/min. Other injuries noted were a large
perineal laceration with an associated
rectal tear and transected posterior
urethra. Anteroposterior pelvic radiograph
showed a Young and Burgess APC III pelvic
fracture. Ultrasound examination showed no
free fluid in the abdomen. Despite receiving
a further two units of PRBCs his SBP dropped
below 90 mmHg and he was taken emergently to
the operating room for combined C-clamp
placement, pelvic packing and laparotomy.
There was significant venous bleeding from
the open perineal wound. The perineal wound
was packed and retroperitoneal packing was
performed through an 8 cm midline incision.
Venous bleeding from the right hemipelvis
was noted upon opening the retroperitoneum.
Laparotomy with diverting sigmoid colostomy,
and suprapubic catheter placement were
performed. The packing and external fixation
procedure consumed 19 minutes. The patient
left the operating room after percutaneous
plate fixation of his femur and urologic
assessment 2 hours and 39 minutes after
arrival in the emergency room.
He was then taken to the surgical intensive
care unit for further resuscitation. Six
days after admission he was taken for
definitive internal and external fixation of
his anterior and posterior pelvis. He
received a total of nine units of PRBCs and
two units of FFP during his hospital stay.
He subsequently underwent delayed rectal and
urethral reconstruction and rehabilitation.
Surgical Technique
The patient is positioned supine. In cases
in which mechanical stabilization is judged
to be advantageous, a C-clamp or external
Fixator is placed using standardized
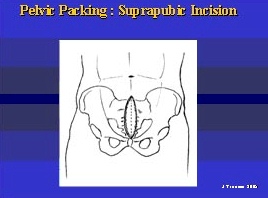
techniques. An 8 cm midline incision is made
extending caudally from the symphysis pubis
in a cephalad direction. Skin and
subcutaneous tissue are sharply incised and
the fascia anterior to the rectus abdominis
is exposed. The fascia is divided in the
midline, the length of the incision. Care is
taken to protect the bladder during incision
as in some cases of symphyseal disruption;
the bladder may be pressed against the
posterior aspect of the abdominal wall. The
bladder is gently retracted to one side with
a malleable retractor and the pelvic brim is
gently palpated from the symphysis in a
posterior direction toward the sacroiliac
joint. In most cases, the fascial
connections of the overlying tissue will
have been dissected free by the force of the
injury. Care should be taken to palpate for
any aberrant vascular connections between
the obturator and iliac systems to avoid
avulsing these vessels (the Corona Mortis).
The pelvic brim is not visualized through
the approach. After the brim has been
palpated as posterior as the surgeon can
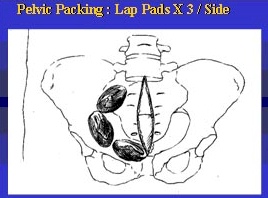
reach, three laparotomy sponges are placed
sequentially deep to the brim. the first is
placed on a sponge stick posterior just
below the sacroiliac joint. The second is
placed anterior to the first sponge at a
point corresponding to the middle of the
pelvic brim. The third sponge is placed in
the retropubic space just deep and lateral
to the bladder. The bladder is then
retracted to the opposite side and the
sequence is repeated until both sides of
the pelvis are symmetrically packed with
three sponges each. The packs should all be
below the pelvic brim in the true pelvis. At
this point, any bleeding evident upon
opening of the retroperitoneum will have
stopped. If bright red bleeding was noted
initially, consideration should be given to
subsequent pelvic angiography either via a
laparotomy by the trauma surgeon or
percutaneously by the interventional
radiologist. The outer fascia is closed with
a single layer running suture to seal the
compartment and the skin incision is
stapled. The total time for the packing
procedure should be under 20 minutes. If
laparotomy is required, it should follow the
closure of the retroperitoneal fascia in
order to preserve the anatomic integrity of
the compartments and to allow for tamponade
in the retroperitoneum. Laparotomy prior to
pelvic packing may result in a difficult
approach into the retroperitoneum and
prolong the overall procedure time. As in
the abdomen, the pelvic packing should be
removed or exchanged at 24-48 hours. Packing
should be removed carefully with saline
added to moisten the packs and lessen blood
clot disruption.
Discussion
Despite advances in management, the
mortality associated with unstable pelvis
fractures remains high. The current emphasis
on embolization does not take into account
the potential mortality of venous bleeding
which is likely present even when arterial
injury occurs. Strategies for control of
venous bleeding consist of external fixation
to enhance pelvic stability and promote
intrapelvic tamponade with graded
resuscitation to prevent coagulopathy. The
addition of direct packing to control venous
bleeding is logical and has been used
effectively in trauma surgery “Damage
Control”, oncologic, gynecologic surgery,
and by Orthopaedic trauma surgeons during
pelvic and acetabular surgery.
In our experience, the procedure can be
performed quickly and the bleeding
encountered when the retroperitoneum is
opened is controllable. The advantage to the
patient is that the volume of ongoing venous
bleeding is decreased early in the course,
allowing the surgical team to concentrate
treatment on associated injuries. The
decreased overall blood loss reduces the
duration of shock and the incidence of
multisystem organ failure (MOF). However, to
be effective, pelvic packing should be
performed early in the course of
resuscitation, preferably within the first
hour of treatment. Following packing the
patient with persistent arterial bleeding
should undergo pelvic angiography or
surgical exploration in order to gain direct
arterial control.
|